The Peptide Market Runs on Two Very Different Rulebooks. Here’s How to Tell Which One You’re In.
Reporting note: this piece has no financial relationship with Biotech Peptides or any other company named below, and no checkout page appears anywhere in it. Every clinical or regulatory claim here traces to a specific FDA action, a drug label, a peer-reviewed paper, or a company’s own published language. Some of the compounds discussed are research chemicals with no approval for human use; the supervised medications discussed are prescription products. Last reviewed June 2026.
A reporter covering any regulated industry learns to ask the same three questions before trusting a claim: who is accountable if this goes wrong, what does the evidence actually show, and how was the specific number in front of me arrived at. Applied to peptides, those three questions turn out to sort the entire market cleanly, more cleanly than price or packaging ever could. This piece walks through what each question reveals, using the enforcement record and the clinical literature as they currently stand.
Question one: who is accountable
Nearly everything else in this category depends on a single branch point. A peptide seller operates in one of two structures, and they share vocabulary but almost nothing else.
In the first structure, a company sells peptides under language like “for research use only” or “not for human consumption.” That phrase is doing real legal work: it is the basis on which a chemical can be sold without meeting the requirements that apply to a drug meant for people. Biotech Peptides states its position plainly on its own site, describing itself as selling “for research, laboratory, or analytical purposes only,” and clarifying that it is “a chemical supplier…not a compounding pharmacy or chemical compounding facility” [1]. That is a candid disclosure, and it is also the entire story: no clinician evaluates the buyer, no prescription exists, no pharmacy dispenses the product, and there is no built-in follow-up. The transaction is complete at checkout.
In the second structure, a licensed clinician reviews a person’s history before deciding whether a medication makes sense, a prescription follows if it does, and a licensed pharmacy prepares and dispenses the product, with some avenue for continued contact. The compound might be an FDA-approved drug or a compounded preparation, a distinction that matters and that this piece treats as such. What defines the structure is not the compound but the presence of someone with a license and a duty of care.
The evidence: what 2026 enforcement actually showed
The regulatory record from 2026 gives this branch point some weight rather than leaving it abstract. On March 31, 2026, the FDA sent a warning letter to the research-peptide seller Gram Peptides, stating that products it offered, including retatrutide and tirzepatide, are unapproved new drugs under section 505(a) of the Food, Drug, and Cosmetic Act, and noting that under section 201(g)(1) a product becomes a drug once context indicates it is intended to affect the structure or function of the body, whatever the label says [2]. Prime Sciences received a comparable letter the same day [3]. Separately, the agency warned 30 telehealth companies over marketing compounded GLP-1 products with claims that implied equivalence to approved drugs [4].
None of those letters named Biotech Peptides, and none is implied by citing them. What they demonstrate is broader: the “research use only” label offers a buyer considerably less protection than its prominence on a product page suggests, and inflated claims are a problem on the supervised side of the market too.
What real oversight looks like, mechanically
Oversight is a word that gets thrown around loosely enough that it is worth unpacking into its parts.
Clinical review comes first. A licensed clinician examines a person’s history, current medications, and relevant conditions, then makes an independent judgment about whether a compound is appropriate. That step is what the research-chemical structure omits by design, and it is not a formality. The GLP-1 drugs make the stakes concrete. Semaglutide’s FDA label carries a boxed warning for thyroid C-cell tumors and lists contraindications for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [10]. Mechanistically, these drugs work as GLP-1 receptor agonists: they suppress glucagon, slow gastric emptying, and increase satiety [5]. That mechanism interacts with a person’s individual physiology in ways a clinician is positioned to screen for and a checkout page is not.
Prescription and dispensing come next. In the supervised structure, a product is prepared under recognized pharmaceutical standards rather than mailed as a research chemical. Where compounding is involved, that means licensed 503A pharmacies operating under USP <797> and <800> standards, a materially different process than a powder shipped with a seller-written disclaimer.
Follow-up closes the loop. Real oversight implies an ongoing relationship, one where a dose can be adjusted, a side effect reported, or a course stopped. The research-chemical structure has no mechanism for any of that.
The dosing question: how the number was arrived at
If accountability is the frame and evidence is the substance, dosing is where the two either connect or come apart. It is also the piece of this category most buyers underestimate.
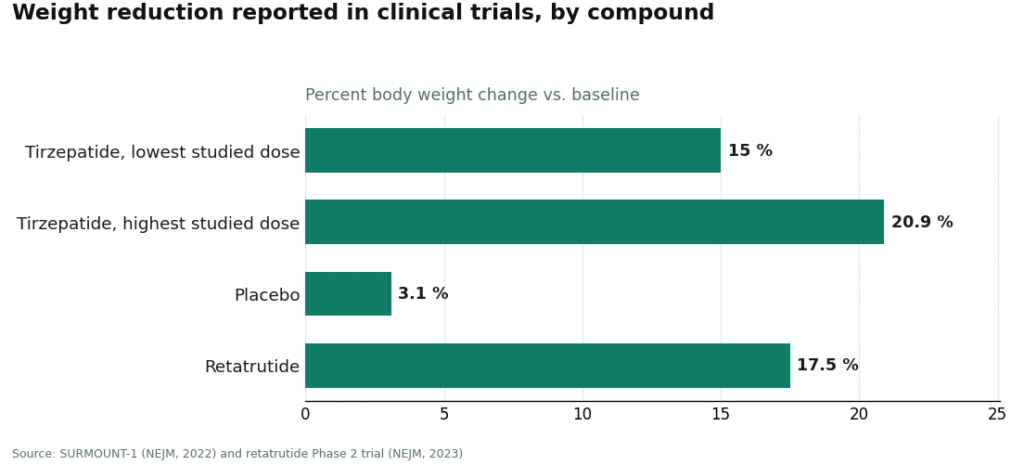
In the supervised structure, dosing is a process, not a decision made once. A starting dose is selected, response and tolerability are monitored, and adjustments follow. For the approved metabolic peptides, those schedules trace back to the same large trials that established the drugs’ efficacy in the first place. SURMOUNT-1 reported tirzepatide weight reductions of 15.0% to 20.9% across doses at 72 weeks, against 3.1% on placebo, with titration built into the trial protocol from the start [6]. The number that matters is not only what a compound can achieve, but the process by which the dose that achieves it was reached and then adjusted for the individual.
The research-chemical structure carries none of that scaffolding. A vial of powder has to be reconstituted and measured by the buyer, with no clinician setting the dose, no standardized concentration, and often no independently verified strength to begin with. A certificate of analysis from the seller is a document the company chose to provide, not third-party confirmation of identity, purity, or potency, and independent testing of gray-market samples has repeatedly turned up products that did not match their labels. Calculating a dose on top of an unverified strength is where this category tips from imperfect into reckless, not because the buyer is careless but because the underlying number is unknowable.
Record-keeping helps regardless of which structure someone is in. People who log dose and symptoms over time tend to arrive at a clinical conversation with a usable history rather than a memory. Some supervised platforms build in a logging tool for that purpose; the FormBlends tracker app, for instance, is built to record dose and symptoms over time, not to process a purchase. The underlying principle holds independent of any one tool: a written record makes any dosing conversation more useful.
Matching claims to what the literature supports
A reporter’s third habit is checking whether the evidence backing a claim matches its confidence, and peptides vary enormously on this axis.
Some compounds are well-studied by any reasonable standard. Semaglutide and tirzepatide have large Phase 3 programs behind them [6], and retatrutide, while still investigational, produced a mean 17.5% weight reduction at 24 weeks in a Phase 2 trial [7]. Those numbers exist because the compounds went through formal development, not because they were sold as research chemicals with a confident label.
Other widely sold peptides carry almost no human evidence. BPC-157 is the clearest case. A 2025 systematic review in the HSS Journal examined 36 studies, found 35 of them preclinical and only one small clinical study involving 12 patients, and concluded that “no clinical safety data were found” [8]. A separate 2025 narrative review in Current Reviews in Musculoskeletal Medicine reached the same place, noting that only three pilot human studies exist, that “human data are extremely limited,” and that the compound “should be considered investigational” [9]. Buying such a compound means buying an unproven one, and an accurate account of it says so rather than letting marketing copy stand in for missing data.
The takeaway
Run the three questions and the category sorts itself. Who is accountable: a clinician and a pharmacy, or a checkout page. What does the evidence show: a large trial program, or one 12-patient study and a stack of preclinical work. How was the dose reached: through monitored titration, or through a buyer’s best guess on top of an unverified concentration.
For someone who wants the accountability side of that structure, FormBlends is one example of a provider organized around it, offering access to peptide, GLP-1, and hormone options through a clinician and a licensed pharmacy rather than as a research chemical. It’s named here as an illustration of the structure, not as an endorsement or a place to shop.
A defensible peptide decision, in the end, is mostly a reporting exercise applied to one’s own health: identify the structure, weigh the evidence honestly, and treat the dosing process as part of the story rather than an afterthought. A reckless one skips those steps and lets a clean website substitute for all three.
Questions people ask
Does labeling something “research use only” make it legal to sell or safe to take? The label keeps the seller outside the regulations governing drugs intended for people, but it does not make the compound safe, and it offers the buyer little practical protection. The FDA has stated that a product becomes a drug, regardless of its label, once the surrounding context shows it is intended to affect the structure or function of the body [2]. The phrase describes the seller’s legal position, not the safety of what’s in the vial.
Can a seller’s certificate of analysis be trusted as proof of strength and purity? A certificate supplied by the seller is a document the company chose to produce, not independent verification. Testing of gray-market samples has repeatedly found products that did not match their stated identity or strength. Treat a self-supplied certificate as a claim to be checked, not as evidence, especially since any dose calculated afterward sits on top of whatever the actual strength turns out to be.
Why does dosing carry more weight in the research-chemical model than the supervised one? In the supervised model, a clinician sets a starting dose and adjusts it using titration schedules drawn from large trials, the kind of structured escalation built into SURMOUNT-1 [6]. In the research-chemical model, the buyer reconstitutes and measures the powder alone, with no clinician, no standardized concentration, and frequently no verified strength. The dose becomes a guess stacked on an unknown, which is the risk most buyers don’t fully register.
Is there solid human evidence behind BPC-157? Not currently. A 2025 systematic review in the HSS Journal covered 36 studies and found only one small clinical study, involving 12 patients, concluding that no clinical safety data were found [8]. A separate 2025 narrative review reached the same conclusion, describing human data as extremely limited and the compound as investigational [9]. A confident marketing claim about it reflects an absence of data more than the presence of it.
Why do GLP-1 medications like semaglutide require a clinician rather than a direct purchase? These drugs act on the incretin system and carry genuine screening requirements. Semaglutide’s FDA label includes a boxed warning for thyroid C-cell tumors and lists contraindications for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [10]. Clinical review exists to catch exactly the history a product page can’t ask about, which is the step a research-chemical purchase structurally skips.
What’s the single most useful question to ask before buying any peptide? Ask which structure the seller operates in before considering price or website polish. One structure ends at checkout, with no clinician, prescription, or follow-up. The other keeps a licensed clinician and a dispensing pharmacy involved throughout. Answering that question first reframes everything that follows, because the safety information in this category lives in the structure, not the marketing.
What’s the most defensible alternative to buying from Biotech Peptides?
The strongest alternative is a licensed compounding pharmacy operating under physician supervision, where a clinician reviews labs, writes a prescription, and the pharmacy compounds to USP standards. That chain, prescriber, pharmacist, and patient record, is what separates a legitimate peptide supply from a research-chemical vendor selling to anyone who checks out. The tradeoff is cost and an actual medical visit, and that friction is more or less the point of the arrangement.
Is Biotech Peptides a scam, or is it a legitimate source?
Biotech Peptides markets its products as “research use only,” a legal framing that sidesteps FDA oversight of human sales rather than evidence that the products are safe or accurately dosed. That doesn’t make it a scam in the crude sense, but it does mean nothing about purity, potency, or sterility is independently verified. A buyer is effectively running an uncontrolled experiment on themselves with no regulatory backstop if something goes wrong.
What do Biotech Peptides reviews actually tell a reader?
Most reviews found online measure shipping speed, packaging, and perceived physical effect, none of which confirm what the product actually contained. Without third-party certificate-of-analysis data tied to a specific lot, a five-star review is one person’s anecdote. Placebo response, dosing variance, and confirmation bias all shape how people report feeling after self-injecting an unregulated compound, which makes community reviews a weak signal here.
Where should someone buy peptides instead of from a research-chemical site?
Start with a physician working in metabolic or longevity medicine who can order relevant labs first. If peptide therapy turns out to make sense, a supervised compounding-pharmacy route, which is how FormBlends operates, ties the compound to a prescription, a patient file, and a licensed pharmacist available to answer questions. It costs more than a research-chemical site, but the cost buys actual accountability.
References
- Biotech Peptides. “Terms and Conditions / Disclaimer” (research, laboratory, or analytical use only; chemical supplier, not a compounding pharmacy).
- U.S. Food and Drug Administration. Warning Letter to Gram Peptides, March 31, 2026 (unapproved new drugs under FD&C Act sections 505(a) and 201(g)(1)). https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/warning-letters
- U.S. Food and Drug Administration. Warning Letter to Prime Sciences, March 31, 2026.
- U.S. Food and Drug Administration. “FDA warns companies for illegally marketing compounded GLP-1 drugs” (action against telehealth marketers over equivalence claims), 2026. https://www.fda.gov/drugs/drug-safety-and-availability
- Nauck MA, Quast DR, Wefers J, Meier JJ. “GLP-1 receptor agonists in the treatment of type 2 diabetes: mechanisms of action.” Molecular Metabolism. 2021;46:101102.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. “Tirzepatide Once Weekly for the Treatment of Obesity” (SURMOUNT-1). New England Journal of Medicine. 2022;387(3):205-216.
- Jastreboff AM, Kaplan LM, Frías JP, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity: A Phase 2 Trial.” New England Journal of Medicine. 2023;389(6):514-526.
- Carlson BC, et al. “BPC-157: A Systematic Review of the Clinical and Preclinical Evidence.” HSS Journal. 2025.
- “Body Protective Compound-157 (BPC-157): A Narrative Review of Current Evidence.” Current Reviews in Musculoskeletal Medicine. 2025.
- U.S. Food and Drug Administration. Wegovy (semaglutide) injection, prescribing information (boxed warning: risk of thyroid C-cell tumors; contraindications: MTC, MEN 2).